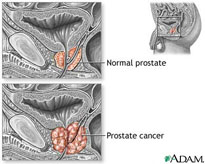
Prostate Cancer
According to the American Cancer Society, there are nearly 200,000 new cases of prostate cancer detected per year, resulting in about 30,000 deaths.1 One in six U.S. men will be diagnosed with prostate cancer and there are about two million men in the country who have been diagnosed with the disease at some point in their lives.2
Understanding Prostate Cancer
Virtually all prostate cancer is initially hormone-sensitive, meaning growth is promoted in the presence of androgens like testosterone and its more potent metabolite dihydrotestosterone.3
Treating Prostate Cancer
The most common pharmacological treatment for the cancer is so-called “androgen-deprivation therapy” or ADT, which aims to lower a patient’s testosterone levels.4 The original non-surgical therapy to accomplish ADT involved the use of estrogens, specifically a synthetic estrogen called diethylstilbestrol or DES.5 DES works by inhibiting the release of gonadotropin-releasing hormone (GnRH) in the brain6 which blocks the gonadal production of testosterone and its metabolites.7 DES, however, became associated with a significant level of thromboembolic and other cardiovascular events.8 Today analogs of GnRH, like leuprolide and other GnRH agonists, are the standard of care for most prostate cancers.9
But GnRH agonists deplete both testosterone and estrogen – testosterone’s natural metabolite. Thus, they are associated with an increased risk of osteoporosis,10 obesity, altered lipid profiles, cardiovascular disease and cardiovascular death, symptoms of metabolic disorder like increased insulin resistance,11 and vasomotor symptoms like “hot flashes.”12
BHR Pharma (BHR) is developing BHR-200 (transdermal estradiol gel) for the palliative treatment of advanced androgen-sensitive carcinoma of the prostate and for the treatment of the vasomotor side effects in men undergoing androgen deprivation therapy (ADT) for prostate cancer. BHR-200 is a prostate cancer treatment that uses a proprietary transdermal estradiol formulation, prescribed alone or in combination with GnRH agonists. Data suggest that by delivering estradiol transdermally, rather than orally, the thromboembolic events seen with earlier estrogen therapies will be substantially mitigated, and the use of estrogen should avoid the bone loss, hot flashes, and several other problems associated with the GnRH agonists.13
1 What Are the Key Statistics About Prostate Cancer?; American Cancer Society.
3 Hormone (Androgen Deprivation) Therapy; American Cancer Society.
5 Crawford, Rev Urol.6 (suppl 7):S3-S11 (2004).
10 Guise et al., Rev Urol. 9:163-180 (2007).
13 Ockrim et al., Nature Clinical Practice Oncology 3:552-63 (2006).